Does Your State Have a Master Plan for Aging?
If not, it should get on the bandwagon.

With the oldest baby boomers turning 85 in just five years, to be followed by some 65 million other members of their generation, the need for elder care in this nation will begin to balloon. The number of these older seniors is projected to grow by more than two and half times from seven million today to a projected 18.6 million in 2050.
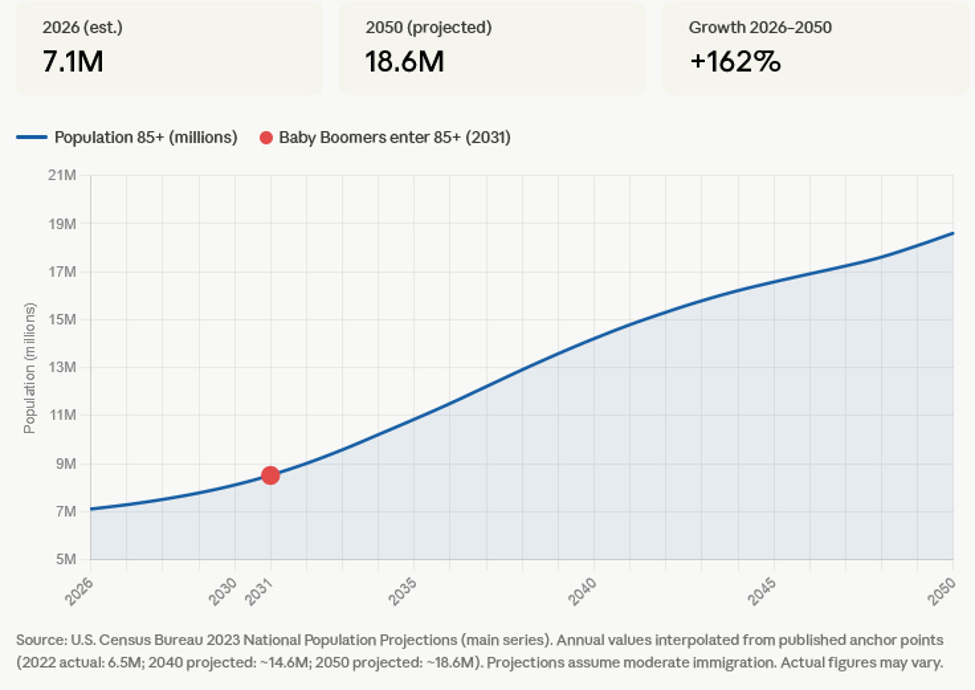
This matters because it’s after age 85 that the need for assistance grows dramatically. And as anyone who has dealt with care needs in their family knows, our cobbled-together elder care system is far from ready. Unfortunately, except in a few states we are not preparing for this totally predictable elder care crisis coming our way.
According to the nonprofit West Health, 14 states have developed master plans for aging. But they are not all equal. For example, my state of Massachusetts has such a plan called ReiMAgine Aging 2030 which, just as its name implies, only runs through 2030. That’s exactly a year before the oldest baby boomers turn 85 so it fails to account for the run up in elder care needs that will begin right then.
State Plans
California, New York and Maryland have longer-range plans that could serve as models for other states.
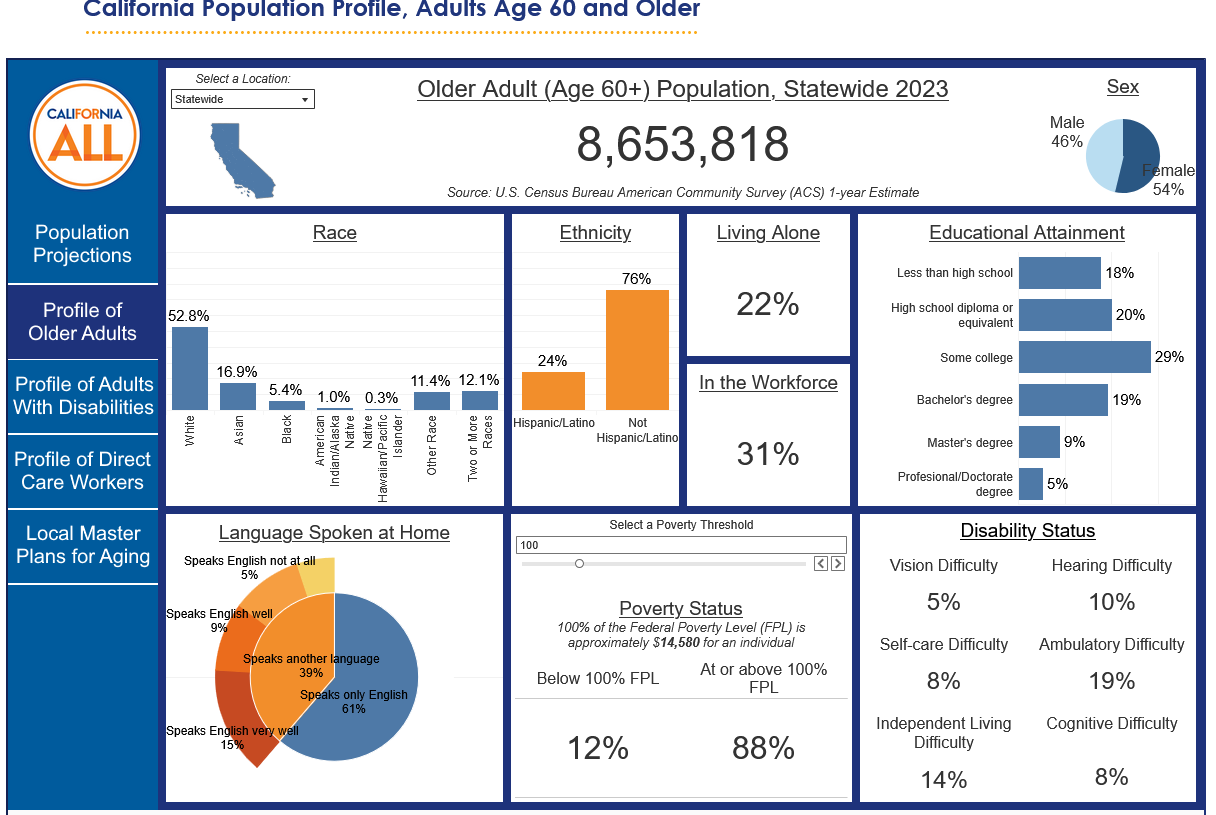
California’s master plan contains five goals involving housing, health, inclusion, caregiving and affordability. One unique feature of the California plan is that it contains a dashboard that provides data on the older population, younger individuals with disabilities and care workers for each county, showing their ethnicity, living situation and poverty status. The state’s department of Health & Human Services issues an annual report on progress towards implementing its aging plan.
Longevity Ready Maryland is a 10-year plan focused on building a longevity ecosystem, promoting economic opportunity, enhancing affordability and optimizing health. At 88 pages, it includes impressive detail about all aspects of the aging infrastructure in Maryland. Like California, it requires an annual report measuring its progress towards plan implementation.
The New York Master Plan for Aging was developed through a “multi-sector” planning process that included government agencies and both nonprofit and for-profit care providers with “the mission of ensuring older New Yorkers and New Yorkers with disabilities can live fulfilling lives, in good health, with freedom, dignity and independence to age in place for as long as possible.” Coming in at some 300 pages with over 100 proposals, the plan is a bit overwhelming. The question is whether such a large number of proposals can be implemented and tracked.
Recognizing the need for all states to follow the lead of these pioneers, Senators Kirsten Gillibrand (D-NY), Angela Alsobrooks (D-MD) and Andy Kim (D-NJ), all members of the Senate Aging committee, have introduced legislation, the Strategic Plan for Aging Act, to fund the development master plans for aging in states around the country.
Multi-Sector Planning
Its focus is on multi-sector planning similar to the New York process because so often seniors, people with disabilities and their families fall through the cracks between the providers of various services, whether hospitals, home health providers, nursing homes or assisted living facilities. Each is working to fulfill its function, often with little communication with the other providers. Coordinated planning has the promise of providing better care at lower cost.
Ben Veghte, executive director of the Washington Cares Fund, conducted a study of the Dutch approach to senior care which is based on multi-sector planning. He explained to me how its experience may be applied to the United States. “We need to invest in this sector, not extract value from it,” he said. “And we really need to realign, restructure the entire long-term care system. That’s where I think looking at other countries that have already cracked the code on this can be really edifying.”
But one of the biggest challenges for multi-sector planning in the United States is that we do not have a single-payer system. European countries spend much more money than the United States on care that keeps people out of hospitals and as a result much less on medical care. This makes sense because the same entities are paying for both.
In the United States, Medicare is designed to pay only for medical care, not for the kind of social care that would keep beneficiaries out of hospitals. In fact, Medicare can only pay for home health care if the patient is homebound and is also receiving some skilled care such as physical or occupational therapy. For those patients who are also covered by Medicaid, it can be confusing and difficult to coordinate because some types of home health care may be covered by one and others by the other, often by two separate entities.
Years ago, Massachusetts had a state-funded Medicare Advocacy Project that assisted residents in qualifying for Medicare coverage of home health and nursing home care, the goal being to shift costs from Medicaid (MassHealth in Massachusetts), which is half state-funded, to Medicare, which is all federal. This just highlights the fact that different providers and funders have different incentives, making coordination difficult which can interfere with the quality of care and increase costs overall.
Coordination and cost sharing can do the opposite — improve quality and reduce costs. But it depends on someone bringing all the players together produce and implement a workable plan. This is where the states need to lead.
Is your state preparing for the inevitable doubling or tripling in the need for elder care? If not, it’s time to get started.
This is a MASSIVE problem heading for a disaster for many elderly. But I question the ability of state governments to tackle it. Government programs tend to be inefficient and end up being more costly or terribly low quality. We owe it to our elders to try to provide a high quality of life to the end. A safety net if you will. This is much more important than the many government programs that are wasteful and corrupt (climate change, “reproductive healthcare” ie abortion-on-demand, homeless enabling, etc).